Affiliated Hospital of Hanzhong Medical College of Science,Taiyuan Shanxi 030000,China
【Abstract】5%of all ovarian tumours are accounted to germ cell tumours(GCT’s).Affecting mostly young women,the highest incidence is seen in second and third decade of life.They are highly malignant but chemosensitive and more curable than their epithelial counterparts.Treating these tumors with effective surgery and combination chemotherapy survival rates have dramatically improved in recent decades.We present our experience of ovarian germ cell tumours in the department of Surgical Oncology,Rajendra Institute of Medical Sciences(RIMS),Ranchi with special emphasis on treatment outcomes.A retrospective review of hospital med-ical records of patients with ovarian germ cell tumours diagnosed and treated at RIMS from June 2019 to August 2020,was performed.Clinical profile and treatment outcome of patients were recorded.A total of 19 patients met criteria.The median age at diagnosis was 20 years(range 11-42 years)and all had good performance status.All except two patients underwent surgery,70.6%and 29.4%in upfront and interval debulking surgery(IDS)setting respectively.Fertility preserving surgery was done in 75%patients in the primary surgery group and 60%undergoing IDS.83.3%patients received BEP as adjuvant chemotherapy whereas 80%as neo-adjuvant chemotherapy.
Majority(31.5%)patients had dysgerminoma as final histology,followed by mixed histology(26.3%),yolk sac tumour(15.7%),immature teratoma(15.7%)and choriocarcinoma(10.5%).47.3%patients were in Stage I at the time of diagnosis.78.9%patients were alive without disease,10.5%recurred,and 10.5%were lost to follow up.
【Keywords】Germ cell tumour;Dysgerminoma;BEP;Fertility sparing surgery;Yolk sac tumour
20 to 25%of all benign and malignant ovarian neo-plasms are of germ cell origin.These are uncommon neoplasms arising from primitive germ cells of the embry-onic gonad.Affecting mostly young women,the highest incidence is seen in second and third decade of life.Most common histology is teratoma followed by dysgerminoma worldwide.
Before mid 1960’s,almost all non-dygerminomatous GCT patients died.The patients with dysgerminoma survived owning to its high radiosensitivity but fertilit was not spared.The introduction of combination che-motherapy VAC(vincristine,dactinomycin,and cyclo-phosphamide)achieved 85%cure rate in stage I GCT’swhereas metastatic disease had a 50-70%[1-2]mortality.Moreover as BEP therapy does not effect ovarian func-tion much,most GCT patients remain fertile and areable to give birth[3-6].FIGO stage and elevated tumour markers are seen to be independent poor prognostic in-
dicators[7].
This is a retrospective study in which data was col-lected prospectively from hospital medical records.All patients with histologically confirmed GCT and treated at RIMS from June 2019 to August 2020 were included.A total number of 19 patients met criteria.
Clinical profile,stage of presentation,histological classification and treatment received(primary surgery followed by chemotherapy or neo-adjuvant chemotherapy
followed by interval debulking surgery)was seen.Treat-ment outcome and disease free interval were ascertained.
The data was analysed using SPSS software.
During this 14 month period,a total of 19 patients were admitted and treated in our department.The median age was 20 years(range 11-42yrs)out of which one patient was premenarchal.All patients had a performance status of ECOG 0/1.The median AFP at presentation was 986ng/mL(range 11-23000 ng/mL),median LDH 843 U/L(range 273-15000 U/L).All except two patients had nor-malβ-hCG(table 1).
Stage wise distribution is depicted in Figure 1.Major-ity patients(n=9;47.3%)belonged to stage I followed by stage III(n=11;26.3%).Two patients belonged to stage II and three to stage IV.
Table 1.Demographics
MedianAge | 20(11-42years) |
PS | Allexcept1wereECOG0/1 |
Tumourmarkersatpresentation | |
AFP | 986(11-23,000) |
LDH | 843(273-15000) |
bHCG | Normalinallexcept2 |

12(70.6%)patients underwent upfront surgery out of which 9(75%)had fertility preservation and 3(25%)had radical surgery.
In terms of adjuvant chemotherapy,10(83.3%)patients received BEP to begin with following which 3(30%)were switched to EP due to bleomycin induced toxicity,2(16.6%)patients received EP,whereas 1(8.3%)received VIP after disease progression on BEP.
Table 3.Interval debulking surgery details
Surgicaldetails:Upfrontsurgery | ||
Type | Details | N=12 |
USO BSO Fertilitypreserved USO/omentum USO/nodes/omentum | 3 1 1 4 | |
Fertilitynotpre-served | TAHBSO TAH BSO/nodes/omentum | 1 2 |
Table 2.Upfront surgery details
Surgicaldetails:Intervaldebulkingsurgery | ||
Type | Details | N=5 |
Fertilitypreservation Fertilitynotpreserved | USO/omental biopsy | 2 |
USO/omentectomy | 1 | |
TAH BSO/omentectomy/LND | 2 | |
7 patients received neo-adjuvant chemotherapy(4 BEP followed by VIP in 1 patient,1 EP and 2 single agent Methotrexate)following which 5 underwent interval debulking surgery(2 patients had choriocarcinoma which was cured with chemotherapy).The reasons for NACT were extensive disease in 2 patients out of which 1 patient also had portal vein thrombosis,poor PS in 2 patients,whereas 1 patient had already received NACT before she presented to us.Among the 5 patients undergoing interval
debulking surgery 3 had fertility preservation.Complete cytoreduction of macroscopic disease was achieved in all patients who underwent surgery.
Among the 10 patients receiving adjuvant BEP che-motherapy following upfront surgery,majority received 4 cycles(6 patients)out of which 2 patients received sub-sequent 2 cycles of EP,3 patients received 3 cycles out of which 1 received subsequent 2 cycles of EP and 1 re-ceived additional 3 cycles of VIP.1 patient was switched to 3 cycles of EP regimen after the first cycle of BEP due to bleomycin toxicity and 2 patients received 4 cycles of EP.
In the interval debulking surgery group,3 patients re-ceived 3 cycles of BEP,1 received 4 cycles BEP whereas 1 received 1st cycle as single agent carboplatin followed by 4 cycles EP as NACT.The patients with choriocarcino-ma received 4 cycles of single agent methotrexate.Post-operatively 2 patients received 2 cycles EP whereas the rest did not need adjuvant treatment.
Table 4.Chemotherapy details
Setting | Regimen | n=19 |
NACT | BEP EP Methotrexate TOTAL BEP | 3 2 2 7 10 |
Adjuvant | EP TOTAL | 2 12 |
Table 5.Chemotherapy cycles
Setting | Cycles | n=40 |
NACT | Three Four Two | 3 4 2 |
Chemotherapy(AfterIDS) | Six Three | 1 2 |
AdjuvantChemotherapy (afterupfrontsurgery) | Four Five Six | 7 1 2 |
19(47.5%)patients had yolk sac tumour,11 patients had mixed histology,5 presented with dysgerminoma,4 with immature teratoma whereas 1 patient had choriocar-cinoma as depicted in figure 2.
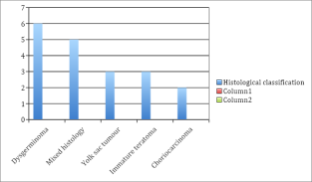
Figure 2.
Follow up data was available for n=17 patients.This data revealed 15 patients alive without disease and 2 pa-tients alive with disease.2 patients developed recurrence and 2 were lost to follow up.None of the patients died during this period.
In the recurrence group,one patient had recurrence in both abdomen and pelvis whereas another one in abdomen and thorax.Both received second-line chemotherapy.Two patients were lost to follow up.
Though accounting for only 5%of all malignant neo-plasms,their impact in patient’s life is enormous since it mostly affects women in their second or third decade of life[8].Fearing the sequelae of the disease,many women choose radical surgery but it has been seen that fertility sparing surgery is also an equally effective treatment with possibility of future childbearing[9].It is now possible to achieve complete cure with fertility preservation however reports on reproductive outcome of GCT survivors are sporadic since it has been only around 30 years since this dramatic improvement due to the implementation of BEP chemotherapy[3-6].However Zhang et al.in their retro-spective study of 32 patients with malignant ovarian germ cell tumour(MOGCT)and sex cord stromal tumours(SCST)showed fertility sparing surgery to be an equally effective alternative to radical surgery with the advantage of menstrual and fertility preservation[10].In their series all patients underwent fertility sparing surgery(FSS)whereas we could achieve 70.5%FSS rate.This could be due to the fact that all except one patient in their series belonged to either stage I or II whereas 42.1%patients in our series had stage III-IV disease.In addition to a desire to cure,a desire to become pregnant also improves treat-ment outcomes[25].
Similarly,Turkmen et al.in their series of 69 patients compared survival outcomes of patients undergoing con-servative surgery with definitive surgery and established surgery type to be insignificant for recurrence[11].Other studies have also shown that fertility sparing surgery did not affect cancer prognosis in cases of advanced germ cell tumours[6,26,27].
Maheshwari A et al.[12]in their report from India,stat-ed dysgerminoma as the most common histological type which is similar to our series of patients.
Though majority of patients belonged to stage I,a con-siderable number of patients presented in the advanced stage.This is due to proper staging surgeries performed at our centre along with late referral from other non-on-cologic treating institutes.Many patients were operated outside without suspicion of malignancy and presented to us with suspicious final histopathology.One patient with advanced disease even received neo-adjuvant chemother-apy outside before presenting to us.BEP chemotherapy is effective for treating germ cell tumors of the ovary and it has been validated in several trials[13-15].
In the NACT setting,there was complete pathologi-cal(or radiological)response in 66.67%patients whereas the rest showed partial response according to the RECIST criteria.S Talukdar et al[16]in their series of 23 patients receiving NACT also showed a complete response of 60.5%.Literature reports 40.7%complete pathological response[17].
10.5%patients recurred and were managed with second line chemotherapy such as VIP(etoposide,ifosfamide,and cisplatin).
Most patients with early disease and healthy looking uterus and ovary underwent fertility sparing surgery.In cases of normal looking contralateral ovary,routine bi-opsy was not taken however it was thoroughly palpated and any suspicious nodules biopsied.Although occult bilaterality has been reported,biopsy of the contralateral ovary could lead to future infertility related to peritoneal adhesions or ovarian failure[18,19].Unlike their epithelial ovarian counterparts,GCT’s are amenable to fertility pres-ervation.Hence it shoud be the standard of care whenever possible.Many studies document good outcome in this regard[20-24].
References
[1]Gershenson DM,Copeland LJ,Kavanagh JJ,Cangir A,Junco GD,Saul PB,et al.Treatment of malignant nondysgerminomatous germ cell tumors of the ovary with vincristine,dactinomycin,and cyclophospha-mide.Cancer,1985,56:2756-61.
[2]Slayton RE,Park RC,Silverberg SG,Shingleton H,Creasman WT,Blessing JA.Vincristine,dactinomy-cin,and cyclophosphamide in the treatment of ma-lignant germ cell tumors of the ovary.A Gynecologic Oncology Group Study(a final report).Cancer,1985,56:243-8.
[3]Gershenson BDM.Menstrual and reproductive func-tion after treatment with combination chemotherapy for malignant ovarian germ cell tumors.Am Soc Clin Oncol,2016,6:270-5.
[4]Brewer BM,Gershenson DM,Herzog CE,et al.Out-come and reproductive function after chemotherapy for ovarian dysgerminoma.J Clin Oncol.,2017,17:2670-5.
[5]Kanazawa K,Suzuki T,Sakumoto K.Treatment of malignant ovarian germ cell tumors with preservation of fertility:reproductive performance after persistent remission.Am J Clin Oncol.,2000,23:244-8.
[6]Tangir J,Zelterman D,MaW,et al.Reproductive function after conservative surgery and chemothera-py for malignant germ cell tumors of the ovary.Ob-stet Gynecol.,2003,101:251-7.
[7]Murugaesu N,Schmid P,Dancey G,et al.Malignant ovarian germ cell tumors:Identification of novel prognostic markers and long term outcome after mul-timodality treatment.J Clin Oncol.,2006,24:4862-4866.
[8]Downey J,McKinney M.The psychiatric status of women presenting for infertility evaluation.Am J Orthop,1992,62:196-198.
[9]Zanetta G,Bonazzi C,Cantu M,Binidagger S,Locatelli A,BratinaG,Mangioni C.Survival and reproductive function after treatment of malignant germ cell ovarian tumors.J Clin Oncol.,2001,19(4):1015-1020.
[10]Zhang N,Chen R,Hua K,Zhang Y.A retrospective study of reproductive outcomes after fertility-spar-ing surgery and postoperative adjuvant chemother-apy in malignant ovarian germ cell tumors and sex cord-stromal tumors.Journal of Ovarian Research,2017,10:52.
[11]Turkmen O,Karalok A,Basaran D,Kimyon G.Fer-tility-Sparing Surgery Should Be the Standard Treat-ment in Patients with Malignant Ovarian Germ Cell Tumors.Journal of Adolescent and Adult Oncology,2017.DOI:10.1089/jayao.2016.0086
[12]Maheshwari A,Gupta S,Parikh PM,Tongaonkar HB.Malignant germ cell tumor ovary-experience at Tata Memorial Hospital.Indian J Med Paediatr On-col.,2004,25(1):43.
[13]Gershenson DM,Morris M,Cangir A,Kavanagh JJ,Stringer CA,Edwards CL,Silva EG,Wharton JT.Treatment of malignant germ cell tumors of the ovary with bleomycin,etoposide and cisplatin.J Clin Oncol.,1990,8(4):715-720.
[14]De Wit R,Roberts JT et al.Equivalence of three or four cycles of bleomycin,etoposide and cisplatin combination therapy and of a 3 or 5 day schedule in good prognosis germ cell cancer:a randomized study of the European Organization for Research and Treatment of Cancer Genitourinary Tract Cancer Co-operative Group and the Medical Research Council.J Clin Oncol.,2001,19(6):1629-1640.
[15]Saxman SB,Finch D,Gonin R,Einhom LH.Longterm follow up of a phase III study of three versusfour cycles of bleomycin,etoposide and cisplatin infavourable prognosis germ cell tumors:the IndianUniversity experience.J Clin Oncol.,1998,16(2):702-706.
[16]Talukdar S,Kumar S,Bhatla N,Mathur S,ThulkarS,Kumar L.Neoadjuvant chemotherapy in the treatment of advanced maligmant germ cell tumors ofovary Gynecologic Oncology,2014,132:28-32.
[17]Culine s,Lhomme C,Kattan J,Michel G,DuvillardP,Droz JP.Cisplatin based chemotherapy in the management of germ cell tumors of the ovary.the InstitutGustave Roussy Experience.Gynecol Oncol.,1997.64(1):160-165.
[18]Gershenson DM.Management of early ovarian cangerm cell and sex cord-stromal tumors.gynecolOnc,199455:s62-72.
[19]Weinstein D,Polishuk WZ.The role of wedge resection of the ovary as a cause for mechanical sterilitySurg Gynecol obstet,1975,141:417-8.
[20]Perrin LC,Lowj.Nicklin Jlwardbg,Crandon AJFertility and ovarian function after conservative sur-gery for germ cell tumors of the ovary.Austn ZJObstet Gynecol,1999,39(2):243-245.
[21]Ezzat A,Raja M,Bakri Y,Subhi J,Memon M,Schwartz P,Stuart R.Malignant ovarian germ celltumors:a survival and prognostic analysiscol,1999.38(4):455-460.
[22]Brewer M,Gerhenson DM.Herzog CE Mitchell MF,Silva EG,Wharton JT.Outcomes and reproductivefunction after chemotherapy for ovarian dysgerminoma.J Clin Oncol.1999.17(9):2670-26.
[23]Park J,Kim D,Suh D,Kim J,Kim Y.Outcomes ofpediatric and adolescent girls with malignant ovariangerm cell tumors,Gynecol Oncol,2015http://dx,doi,org/10.1016/j.ygyn9.2015.03.054.
[24 Weinberg L,Lurain J,Singh D,Schink J,Survivaland reproductive outcomes in women treated formalignant ovarian germ cell tumors.GynecologicOncology,2011,121:285-289.
[25]Tamauchi S,Kajiyama H,Yoshihara M Ieda Y,Yoshikawa N,Nishino K Utsumi F.Niimi K SuzukiS,Kikkawa F.Reproductive outcomes of 105 malig-nant ovarian germ cell tumor survivors:a multicenterstudy.Am J Obstet Gymecol,2018,219(4):385 e1385.e7DOE 10.1016j-ajog 2018.07.021 Epub 2018 Aug 4PMID-30086295.
[26]Patterson DM,Murugaesu N,Holden L,et al.Areview of the close surveillance policy for stage Ifemale germ cell tumors of the ovary and other sitesInt J Gyneco!Cancer,2008,18:43-50.
[27]Park J Y,Kim D Y,Suh D S,et al.Analysis of outcomes and prognostic factors after fertility-sparingsurgery in malignant ovarian germ cell tumors.Gynecol Oncol.2017.145:513-8.

客服QQ:30444492琼网文【2021】1550-113号
增值电信业务经营许可证:琼B2-20210322
出版物经营许可证:新出发龙华出字第(2021)009号
广播电视节目制作经营许可证:(琼)字第00779号
版权所有 ©2002-2024 期刊网 琼ICP备2021005105号