Tianjin Binhai New Area Hospital,Tianjin 300457,China
【Abstract】Objective:There are limited data in the literature regarding the potential relationship between thyroid cancer and ABO blood types and Rh factor.The aim of our study was to investigate whether papillary thyroid cancer(PTC)is associated with blood type.Materials and Methods:The present study included patients who pre-sented to Dicle University Faculty of Medicine between June 2009 and December 2020 and were diagnosed with PTC as a result of postoperative(thyroidectomy)histopathological analysis.The control group consisted of inpiduals whose blood type was analyzed at a random blood center.Results:Of the 223 patients diagnosed with PTC,163(73.1%)were fe-males and 60(26.9%)were males.In the comparison of patients based on ABO blood types and Rh factor,A Rh positive blood type was found 31%less frequently in the PTC group compared with the control group,and thus it was associated with a lower risk of PTC(OR:0.69;95%Confidence In-terval:0.50–0.96,p=0.029).Conclusions:In our study,we found A Rh positive blood type to be signifi-cantly less frequent among patients with PTC.A Rh positive blood type can be considered as a protective factor indicating a reduced risk of PTC.
【Keywords】Papillary thyroid cancer;Blood types;ABO;Rh
Thyroid cancers are the most common endocrine ma-lignancy and account for approximately 3%of the global cancer incidence[1].Differentiated thyroid cancers(DTCs)arising from thyroid follicular epithelial cells account for the vast majority of thyroid cancers.A total of 3%–9%of DTCs are familial[2],and approximately 85%of these DTCs are papillary thyroid cancers(PTCs)[3].Increased incidence rates are mainly due to increased PTC diagnosis rates.Detection of small and subclinical PTCs has become easier with the improvements in imaging techniques,biopsy methods(fine needle aspiration biopsy),medical surveillance,and healthcare accessibility[4].Therefore,the incidence of thyroid cancer is still increasing[5].
The well-known risk factor for the development of thy-roid cancers,particularly PTC,is exposure to ionizing ra-diation,particularly during childhood[2,6-9];however,it is considered that other factors(family history,sex,obesity,smoking,alcohol consumption,hormonal exposure,and some environmental pollutants)may also play a role[1,9,10].It is believed that exposure to certain chemicals during intrauterine life and early childhood,especially along with possible epigenetic changes,may result in a muta-genic tendency in thyroid cells[6].An inverse relationship between smoking and alcohol consumption and thyroid cancer has been mentioned in some studies[9,10].Other factors that are believed to cause thyroid cancer include high dietary iodine content(especially PTC)[8],as well as intakes of selenium,goitrogens,and carcinogens.High thyroid stimulating hormone levels and genetic syndromes(Gardner,Cowden,and Werner syndromes)have been as-sociated with DTC[7].Because most flame retardants have chemical structures similar to thyroid hormones,they have been reported to alter thyroid hormone homeostasis and have ultimately become one of the suggested causes owing to their potential effects on the risk of thyroid can-
[10]
cer.
Blood type analysis is a key procedure in the blood transfusion process along with genetic analyses and asso-ciated disease examinations.The first blood type antigen system was the ABO system[11].ABO blood type antigens are defined by the carbohydrate moieties on the outer sur-face of the erythrocyte cell membrane[12].ABO antigens are also secreted from many sites other than erythrocytes,including platelets,vascular endothelial cells,mucous,and epithelial tissues[13].The Rh system is the second most important blood type system in the preliminary transfusion test[11].
Clinical studies have shown that the ABO blood type plays a role in various diseases and malignancies[14].The relationship between ABO blood types and cancer was first reported in 1953.Since then,numerous studies have been published with often conflicting results[13].Although some studies evince a relationship between ABO blood type antigens and various cancer types,there is limited data on its prognostic significance in patients[12].Further large-scale studies are warranted to determine whether ABO antigens have a function and,if they do,how this function contributes to tumorigenesis[13].In this study,we aimed to determine whether PTC,a type of DTC,is asso-ciated with blood type.
2.Materials and Methods
Patients who presented to Dicle University Faculty of Medicine between June 2009 and December 2020 and were diagnosed with PTC as a result of postoperative(thyroidectomy)histopathological analysis and a control group consisting of inpiduals whose blood type was analyzed at a random blood center were retrospectively included in the present study.
The control group consists of people who applied to the emergency department of our hospital between these dates for any reason and whose blood groups were studied in the blood center.Inpiduals were selected by simple randomization to avoid bias from the hospital system.No disease screening was performed in the control group.Adults older than 16 years were included in the control group.It is known that the prevalence of thyroid diseases is higher in female gender.Therefore,gender matching was not done between the groups so that the control group represents the real population.
The blood types of these inpiduals were recorded.ABO and Rh blood types were determined at the blood center using the gel centrifugation method(column ag-glutination;Ortho AUTOVUE INNOVA).Inpiduals aged<16 years,patients with concomitant non-thyroid malignancies,and those other non-ptc thyroid ma-lignancies were excluded from our study.this study was approved by dicle university medical ethics committee(no:145>
The data were analyzed using SPSS Version 22.The control and PTC groups were compared.Chi-square test was used to compare categorical variables and Mann-Whitney U test was used to compare numerical variables between groups.For statistical significance,re-sults with p<0.05 at 95%Confidence Interval(CI)were considered significant.
3.Results
Of the 223 patients with PTC in the study,163(73.1%)were females and 60(26.9%)were males.Their median age(minimum–maximum)was 43(16–86)years.Of the 1040 inpiduals in the control group,547(52.6%)were females and 493(47.4%)were males.Their median age(minimum–maximum)was also 43(16–90)years.PTC was observed at a significantly higher rate in females(p<0.001).A comparison based on ABO blood types and Rh factor revealed that A Rh positive blood type was ob-served at a lower rate in the PTC group than in the control
group(OR:0.69;95%CI:0.50–0.96,p=0.029).However,there were no significant differences among other blood types and Rh factors.The occurrence rates of blood types in the PTC and control groups and the demographic char-acteristics of the inpiduals are presented in Table 1.
Although A blood type was the most common blood type in Diyarbakir,Turkey(control group),with an oc-currence rate of 37.6%,O blood type was found to be the most common blood type in the PTC group,with an oc-currence rate of 38.6%.Percentage distributions of blood types are presented in Figure 1.In Figure 2,the distribu-tions of ABO blood types and Rh factor in the PTC and control groups are presented.A Rh positive blood type was found at an occurrence rate of 33.6%in the control group and 26%in the PTC group,whereas O Rh positive blood type was found at an occurrence rate of 32.1%in the control group and 35%in the PTC group.
Table 1.Distribution ofABO blood types and Rh factor in the control and papillary thyroid cancer groups
PTC n=223(%) | Control n=1040(%) | pvalue | |
Age(years)* | 43(16̶86) | 43(16̶90) | 0.261 |
Sex | |||
Female | 163(73.1%) | 547(52.6%) | <0.001 |
Male | 60(26.9%) | 493(47.4%) | <0.001 |
ABO | |||
APositive | 58(26%) | 349(33.6%) | 0.029 |
ANegative | 10(4.5%) | 42(4%) | 0.761 |
BPositive | 40(17.9%) | 172(16.5%) | 0.612 |
BNegative | 10(4.5%) | 27(2.6%) | 0.129 |
ABPositive | 16(7.2%) | 74(7.1%) | 0.975 |
ABNegative | 3(1.3%) | 12(1.2%) | 0.811 |
OPositive | 78(35%) | 334(32.1%) | 0.408 |
ONegative | 8(3.6%) | 30(2.9%) | 0.577 |
Rhfactor | |||
RhPositive | 192(86.1%) | 929(89.3%) | 0.229 |
RhNegative | 31(13.9%) | 111(10.7%) | 0.575 |
PTC:Papillary thyroid cancer;p<0.05 was considered statistically significant.*Median(minimum–maximum)
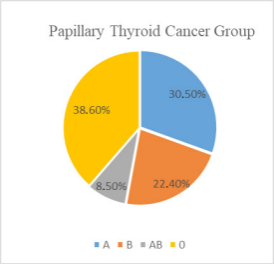

Figure 1.Schematic distribution ofABO blood types

Figure 2.Occurrence rates ofABO blood types and Rh factor in the thyroid papillary cancer and control groups(in percentages)
4.Discussion
Over 90%of thyroid cancers are of the follicular or pa-pillary variants often termed differentiated thyroid cancer[15].Many factors other than ionizing radiation have been reported to be associated with the etiology of thyroid can-cer,but a definite causality has not yet been established.There are limited data in the literature regarding the pos-sible relationship between thyroid cancer and ABO blood types and the Rh factor[14].Blood types have been inves-tigated in the etiology of many malignancies.Meta-analy-ses have detected a decreased risk of gastric,pancreatic,breast,ovarian,colorectal,esophageal and nasophary-ngeal cancers for patients with O blood type.Although associations between some malignancies and blood types have been demonstrated,the link between the expression of blood type antigens and tumor formation has not been clarified for most tumor types in various studies.It was thought that genome-wide association studies may provide prognostic support for the association between the ABO glycosyltransferase gene and cancer risk[13].In a study,blood group A was associated with significantly higher risk for malignancy including hepatocellular carcinoma,pancreatic and breast cancers while biliary and esophageal cancer risk was significantly associated with blood type B[16].In another study both B and AB blood types have been associated with a significantly lower risk of gastro-intestinal cancer,colorectal cancer.Blood group B was also associated with a significantly lower risk of stomach cancer and bladder cancer,while blood group AB was observed to significantly increase the risk of liver cancer.It has been found that the risk of gastric cancer,colorectal cancer increases with blood group A[17].We investigated the relationship between PTC and blood types in the pres-ent study.
The distribution of ABO blood types and Rh factor var-ies between populations and races[18].In a research con-ducted in Diyarbakir in Turkey,ABO and Rh blood type ratios were found to be similar to our study.The blood groups of a total of 206.673 people who applied to blood centers were found respectively;36.55%A Rh(+),29.70%
O Rh(+),16.65%B Rh(+),6.26%AB Rh(+),4.26%A Rh(–),3.95%O Rh(–),1.88%B Rh(–),0.72%AB Rh(–).89.17%of the applicants were Rh positive and 10.82%were Rh negative.As a result,it was stated that there were few differences with the blood group distributions in other regions of our country,and the blood group distribution determined in the study was similar to our country in general[19].In the present study,the A blood type was the most common blood type,with a slightly higher occur-rence rate than the O blood type,which was found at a similar rate to the control group.In the PTC group,blood type A was observed less frequently,whereas blood type O was observed relatively more frequently.The lower oc-currence rate of A blood type was statistically significant;however,the higher occurrence rate of O blood type was not statistically significant.
Recent studies have reported a relationship between polymorphisms in the ABO gene locus and circulating tumor necrosis factor-alpha,intercellular adhesion mole-cule-1,E-selectin,and P-selectin levels.It is considered that altered ABO glycosyltransferase activity affects cell proliferation,tumor invasion,and metastatic invasion,thereby playing a key role in carcinogenesis.This suggest-ed that ABO blood type may directly influence tumorigen-esis and tumor spread and provide a biological basis for its putative effect on cancer survival.The results of studies evaluating the prognostic significance of ABO antigens in various cancers are rather contradictory.Blood type O appears to be protective against cancer development and progression in pancreatic cancer,whereas the expression of A blood type antigen in tumor cells is reportedly a pos-itive prognostic factor in lung cancer[12].In our study,A Rh positive blood type was found to be a positive protec-tive factor for PTC.
There are limited data in the literature regarding the relationship between blood types and Rh factor in thyroid cancer.Initially,the keratan sulfate epitope was consid-ered as a specific marker of PTC cells and was observed to be produced simultaneously with poly-N-acetyllac-tosamine,which carries blood type antigens[20].In another study,the expression of blood type-related antigens was demonstrated in thyroid follicular epithelial cells[21].In a similar study,it was reported that the neoplastic trans-formation of thyroid gland was accompanied by progres-sive re-expression of blood type-related antigens,which are not found in normal tissues.The results of that study suggested that poly-N-acetyllactosamine structures are produced in papillary carcinomas in a linear fashion,and these structures are of promising diagnostic value for dis-tinguishing PTC from other thyroid malignancies[22].Be-cause of these findings that support the role of blood type in cancer pathogenesis,it is believed that there may be a relationship particularly between PTC and blood type.
In a study investigating the relationship between thy-roid cancer,diabetes,and ABO blood type[23],87 patients with thyroid cancer(68 of them had PTC)were compared with a control group.The most common blood type was O in both groups.It was observed that,compared with the control group,blood type A was significantly less common in patients of 60%)thyroid cancer risk was reported in patients with blood type B.It was considered that blood type A could significantly reduce the risk of thyroid cancer,whereas blood type B could increase this risk.However,there was no significant relationship between PTC and ABO blood type.The low number of patients with PTC in that study may explain the inability to reveal any relationship with blood type A.As a matter of fact,we found that the risk of PTC decreased significantly by 31%in patients with A Rh positive blood type in our study(OR:0.69,95%CI:0.50–0.96).In addition,in the present study,although blood type B was found to be relatively more common in the PTC group,this increase was not statistically signifi-cant.
In another study evaluating Rh factor together with ABO blood types[14],1299 patients with benign and 744 patients with malignant thyroid disease(700 of them had PTC)were compared based on their histopathological fea-tures.Inpiduals with malignant disease were more fre-quently Rh positive than inpiduals with benign disease.However,no significant relationship was noted between ABO blood types and thyroid malignancy.Blood type B was considered to potentially contribute to the develop-ment of thyroid cancer and as a risk factor for autoimmune thyroid disease.It was considered that the aforementioned study was not sufficient to evaluate the differences in blood types of patients with thyroid cancers and the nor-mal population because it only compared patients with benign thyroid disease and those with malignant thyroid disease.In our study,no significant difference was found between the PTC group and the control group in terms of blood Rh factor.
The limitation of our study in cancer risk assessment was the inability to evaluate the genetic transition of PTC and the environmental exposure of the patients because it was a single-centered,retrospective study.
In conclusion,genetic transitions and potential expo-sure to environmental carcinogens and ionizing radiation are considered to be the main factors responsible for the pathogenesis of thyroid cancer.However,A Rh positive blood type can be considered as a protective factor indi-cating a reduced risk of occurrence of PTC.
References
[1]Gallardo,E.,Medina,J.,Sánchez,J.C.,Viúdez,A.,Grande,E.,Porras,I.,Ramón,Y.,Cajal,T.,Trigo,with thyroid cancer and reduced the risk of thyroid cancer by 43%.Borderline(increased risk J.,Iglesias,L.,Capdevila,J.,2020.SEOM clinical guideline thyroid cancer.Clin Transl Oncol.22(2),223-35.
[2]Fagin,J.A.,Wells,S.A.Jr.,2016.Biologic and Clin-ical Perspectives on Thyroid Cancer.N Engl J Med.375(11),1054-67.
[3]Haugen,B.R.,Alexander,E.K.,Bible,K.C.,et al.,2016.American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer:The American Thyroid Association Guidelines Task Force on Thy-roid Nodules and Differentiated Thyroid Cancer.Thyroid.26(1),1-133.
[4]Filetti,S.,Durante,C.,Hartl,D.,Leboulleux,S.,Locati,L.D.,Newbold,K.,Papotti,M.G.,Berruti,A.,2019.Thyroid cancer:ESMO Clinical Practice Guidelines for diagnosis,treatment and follow-up†.Ann Oncol.30(12),1856-83.
[5]Cabanillas,M.E.,McFadden,D.G.,Durante,C.,2016.Thyroid cancer.Lancet.388(10061),2783-95.
[6]Pellegriti,G.,Frasca,F.,Regalbuto,C.,Squatrito,S.,Vigneri,R.,2013.Worldwide increasing incidence of thyroid cancer:update on epidemiology and risk factors.J Cancer Epidemiol.965212.
[7]Schneider,D.F.,Chen,H.,2013.New developmentsin the diagnosis and treatment of thyroid cancer.CA Cancer J Clin.63(6),374-94.
[8]Ain,K.B.,1995.Papillary thyroid carcinoma.Etiol-ogy,assessment,and therapy.Endocrinol Metab Clin North Am.24(4),711-60.
[9]Sadeghi,H.,Rafei,M.,Bahrami,M.,Haghdoost,A.,Shabani,Y.,2018.Attributable risk fraction of four lifestyle risk factors of thyroid cancer:a meta-analy-sis.J Public Health(Oxf).40(2),e91-e98.
[10]Seib,C.D.,Sosa,J.A.,2019.Evolving Understanding of the Epidemiology of Thyroid Cancer.Endocrinol Metab Clin North Am.48(1),23-35.
[11]Dzieczkowski,J.F.,Anderson,K.C.,2011.Transfu-sion Biology and Therapy.Harrison’s Principles of Internal Medicine.Longo DL,Kasper DL,Jameson JL,Fauci AS,Hauser SL,Loscalzo J(eds).18th ed.New York.McGraw-Hill Education.(1),951-7.
[12]Franchini,M.,Liumbruno,G.M.,Lippi,G.,2016.The prognostic value of ABO blood group in cancer patients.Blood Transfus.14(5),434-40.
[13]Rummel,S.K.,Ellsworth,R.E.,2016.The role of the histoblood ABO group in cancer.Future Sci OA.2(2),FSO107.
[14]Tam,A.A.,Özdemir,D.,Fakı,S.,Bilginer,M.C.,Ersoy,R.,Çakır,B.,2020.ABO Blood Groups,Rh Factor,and Thyroid Cancer Risk:To‘B’or Not to‘B’Endocr Res.45(2),137-46.
[15]Nix,P.,Nicolaides,A.,Coatesworth,A.P.,2005.Thy-roid cancer review 2:management of differentiated thyroid cancers.Int J Clin Pract.59(12),1459-63.
[16]Mansour,A.,Mohammed,M.A.,Anwar,R.,Elzaf-rany,M.,Omar,N.M.,2014.ABO blood group and risk of malignancies in Egyptians.Int J Cancer Res.10(2),81-95.
[17]Huang,J.Y.,Wang,R.,Gao,Y.T.,Yuan,J.M.,2017.ABO blood type and the risk of cancer-Findings from the Shanghai Cohort Study.PLoS One.12(9),e0184295.
[18]Kumar,S.,Modak,P.K.,Ali,S.H.,Barpanda,S.K.,Gusain,V.S.,Roy,R.,2018.A retrospective study:ABO and Rh phenotype blood group distribution among blood donors in H.N.B.Base Hospital,Sri-nagar,Uttarakhand,India.J Family Med Prim Care.7(1),34-8.
[19]Temiz,H.,Altıntaş,A.,Gül,K.,2008.Distribution of ABO and Rh Blood Groups in Diyarbakir.Interna-tional Journal of Hematology and Oncology.4(18),234-7.
[20]Ito,N.,Yokota,M.,Nagaike,C.,Morimura,Y.,Ha-take,K.,Tanaka,O.,Matsunaga,T.,1996.Simulta-neous expression of keratan sulphate epitope(a sul-phated poly-N-acetyllactosamine)and blood group ABH antigens in papillary carcinomas of the human thyroid gland.Histochem J.28(9),613-23.
[21]González-Cámpora,R.,García-Sanatana,J.A.,JordàiHeras,M.M.,Salaverri,C.O.,Vázquez-Ramírez,F.J.,Argueta-Manzano,O.E.,Galera-Davidson,H.,1998.Blood group antigens in differentiated thyroid neoplasms.Arch Pathol Lab Med.122(11),957-65.
[22]Yokota,M.,Ito,N.,Hirota,T.,Yane,K.,Tanaka,O.,Miyahara,H.,Matsunaga,T.,1995.Histochemical differences of the lectin affinities of backbone poly-lactosamine structures carrying the ABO blood group antigens in papillary carcinoma and other types of thyroid neoplasm.Histochem J.27(2),139-47.
[23]Khoshsirat,S.,Peyvandi,A.A.,Oroei,M.,Peyvandi,H.,Rezaeifard,A.,2019.The Estimation of Thyroid Cancer Risk based on Type 2 Diabetes Mellitus and ABO Blood Group.Turk J Oncol.35(1),64-9.

客服QQ:30444492琼网文【2021】1550-113号
增值电信业务经营许可证:琼B2-20210322
出版物经营许可证:新出发龙华出字第(2021)009号
广播电视节目制作经营许可证:(琼)字第00779号
版权所有 ©2002-2024 期刊网(www.qikanchina.com) 琼ICP备2021005105号